AUCTORES
Globalize your Research

Case report | DOI: https://doi.org/10.31579/2578-8949/033
*Corresponding Author: M. Napolitano, Departimento di Medicina e Scienze della Salute
Citation: M. Napolitano , T. Cirillo , C. Patruno , P. Gisonni, M. Megna , N. Balato, 2018, 10 Frequent Diagnosis in Dermatology. J .Dermatology and Dermatitis DOI:10.31579/2578-8949/033
Copyright: © 2018 M. Napolitano, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 March 2018 | Accepted: 08 May 2018 | Published: 21 May 2018
Keywords: Phototherapy; Inflammatory disorders; Nail disorders; Corticosteroid-topical
Abstract
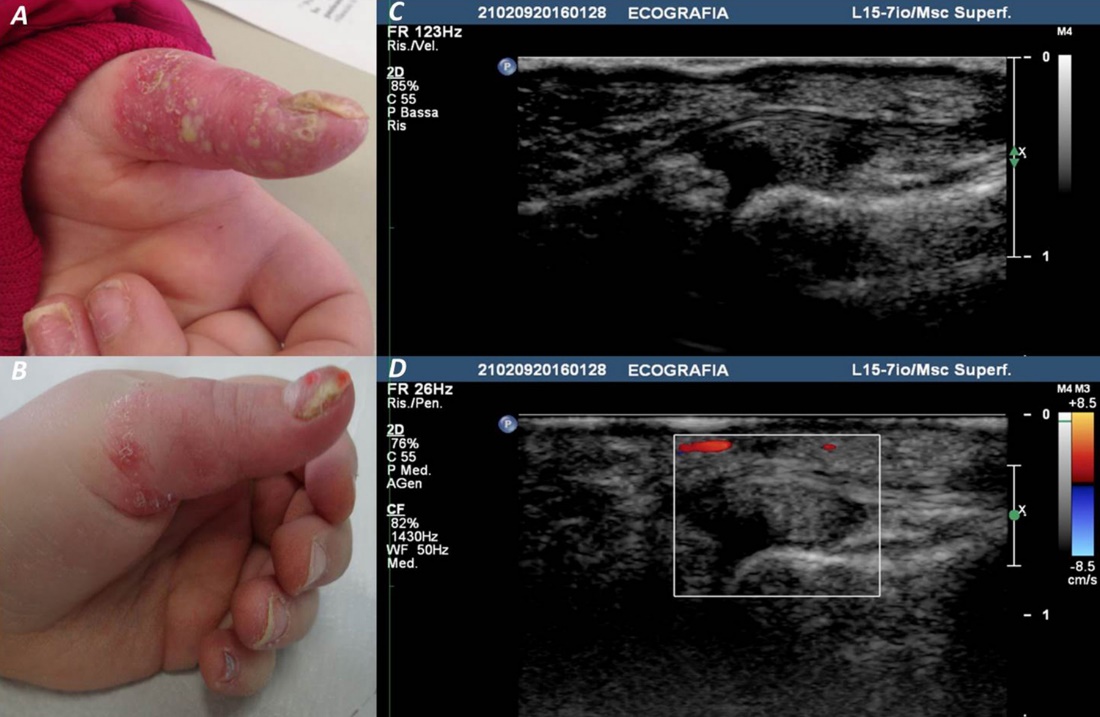
A 6-year-old girl presented to our attention with a 7-month history of erythema and pustules on the distal portion of her left first finger, which deeply affected the beginning of her scholar activity. On examination, her digit was swollen, markedly erythematous, and littered with several small pustules; nail was strikingly dysmorphic. The other digits showed variable degree of onychodystrophy (Fig. 1A). There were neither prior history of psoriatic lesions nor familiarity for psoriasis. Microscopic and cultural examination did not show any microbiological infection. Histological sample showed psoriasiform hyperplasia, with a collection of granulocytes in the context of parakeratosis as well as in the intraepithelial area (Munro-like microabscesses), and focal spongiosis with absent granular layer. The dermis showed increased vascularity within the dermal papillae. Ultrasonography highlighted cutaneous and sub-cutaneous thickness increase with intra-articular synovial effusion (Fig. 1C); at color Doppler, increase of vascularization was present in sub-cutaneous tissue (Fig. 1D). On the basis of these findings, a diagnosis of acrodermatitis continua of Hallopeau (ACH) was performed. Past treatment only consisted of topical steroids. A cycle of clobetasol 0.05% ointment under occlusion and narrow band UVB (310 -311 nm) was prescribed for 30 days. The improvement observed at follow-up visit (Fig. 1B), increased after the subsequent 2 months of therapy, without relapse. The young patient is still under treatment and no relapse was notead at 3.5 months follow-up.
ACH is a rare chronic recurrent skin disorder, characterized by pustular eruption on the distal phalanges of fingers and toes. Involvement of the nail bed and matrix often leads to onychodystrophy, and even to anonychia (1). In a later stage, ACH may lead to osteolysis of the distal phalanges, perceived as joint pain and stiffness (1). Some authors consider ACH as a variant of pustular psoriasis, but others classify it as a separate entity (1). The disease mainly affects middle-aged women whereas is rare in childhood (1).
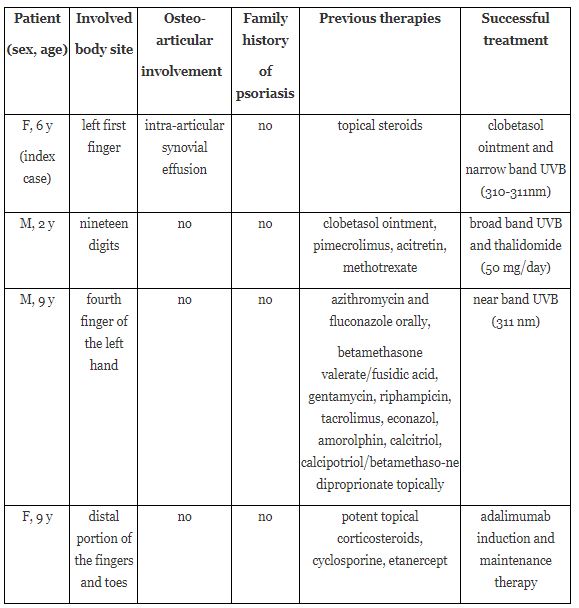
Treatment of ACH can be a challenge, because the use of many therapeutic alternatives has drawbacks or is off-label in childhood. Phototherapy is a well-tolerated treatment for many childhood dermatoses, and is especially efficacious for recalcitrant skin disorders, such as psoriasis (2). Literature reports only 3 cases of ACH in children, all refractory to previous therapies; in particular, the efficacy of phototherapy, alone or in association with tacrolimus, was reported in 2 cases, while in the third case report, phototherapy use was not attempted (3-5) (Table 1).
Also our little patient benefitted from a therapy regimen including phototherapy plus clobetasol ointment; however, only 3.5 months of follow-up have been performed until now. Moreover, as absenteeism from school for patients as well as loss of working days for their attendants are a significant challenge in this treatment modality, we performed phototherapy sessions in the late afternoon.
In conclusion, phototherapy might be considered in pediatric patients with ADH who failed previous topical and/or systemic therapies. Nevertheless, as already performed for more common childhood disease, such as psoriasis and atopic dermatitis, studies deepening the use of phototherapy should be performed also for pediatric ACH. The absence of treatment guidelines is attributed to a lack of controlled studies, which is justifiable by the infrequency of the illness. Many therapeutic modalities have been used for ACH with equivocal results. These include topical preparations such as corticosteroids, calcineurin inhibitors, and vitamin D analogs. Moreover, many reports have evaluated the use of systemic therapies, including immunosuppressive medications and biological therapy, with variable results (6,7). Since ACH is considered a variant of psoriasis, it is assumed that inhibition of tumor necrosis factor α could achieve a successful response (6).
Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.





























































